When it comes to consumer genetics testing, 23andMe ranks at the top. Here, we give...
Read More
When it comes to consumer genetics testing, 23andMe ranks at the top. Here, we give...
Read More
The best online doctor and medical services in 2023; include industry staples like Teladoc and...
Read More
For years, HairClub's been offering lifelines for those with hair loss, but are their hair...
Read More
Walgreens is one of America's leading pharmacy chains, but does their app meet the expectations...
Read More
K Health is shaping the future of healthcare with its affordable pricing and innovative approach;...
Read More
Everlywell is a telehealth company that offers affordable at-home testing kits for tons of health...
Read More
Nurx is a telemedicine company that could help you get medications easier than visiting your...
Read More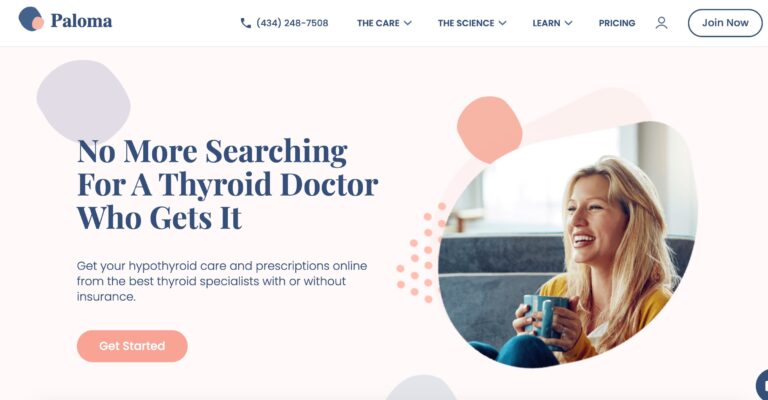
Paloma Health's at-home thyroid test offers an easy way to diagnose potential thyroid conditions; but...
Read MoreAt-home testing for STDs and other health concerns is growing increasingly popular, but myLAB Box...
Read More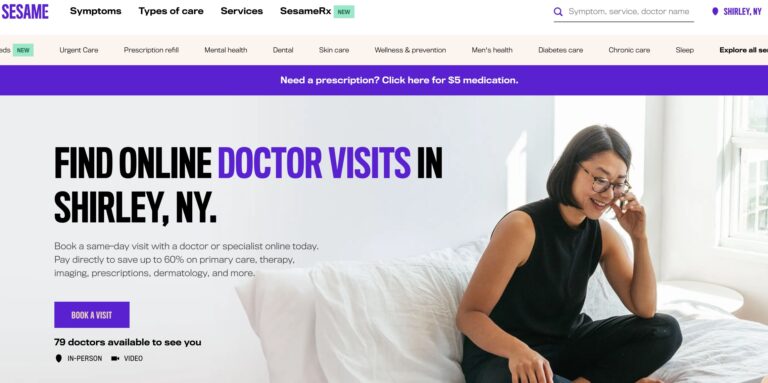
Sesame is a direct-to-consumer telemedicine company that offers a variety of services for a single,...
Read More
If you’re looking for the best hair loss treatment for men, look no further than...
Read More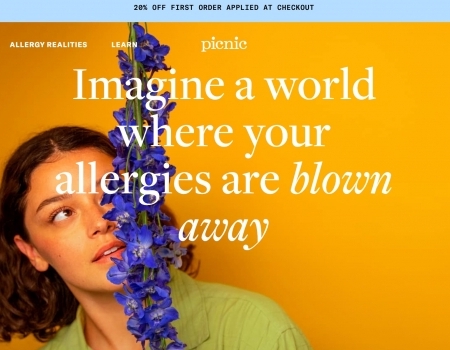
Picnic is a telehealth company that provides personalized treatment for allergy relief, but do they...
Read More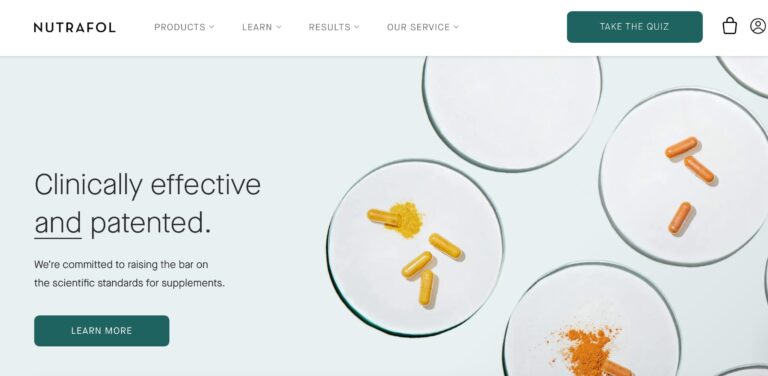
Nutrafol is a telehealth company that offers a range of hair supplements for both men...
Read More
Teladoc is a direct to consumer healthcare company that offers medical care online or via...
Read More
Lemonaid Health is one company looking to bring affordable telemedicine to all. Here are a...
Read More
At-home STD test options range from fully online options to tests that require a visit...
Read MoreShapiro MD uses natural DHT blockers in its shampoos, conditioners, and topical treatments, which may...
Read More
Considering at-home testing? LetsGetChecked is a great resource. Learn how this company works and what...
Read More
Exploring Pharmacy Density Nationwide
Read More
We’ve surveyed over 1,000 people to get their takes on this latest political controversy surrounding...
Read More
Let’s take a closer look at how many Americans report using different drugs (including marijuana,...
Read More
Have you ever lied to your doctor? If your answer is yes, don’t worry, you’re...
Read More
Shouldn’t vaccinations, ambulance rides, and diapers be free? We surveyed 1,000+ Americans to uncover which...
Read More
To determine if people trust AI for medical and health advice, we surveyed 1,015 participants...
Read More